13 Trauma - Arterial
Authors: Kevin Kniery, Adham Elmously, Nakia Sarad, and Todd Rasmussen
These trauma episodes were developed in collaboration with Behind the Knife: The Premier Surgery Podcast.
Vascular trauma requires close collaboration between vascular surgeons and trauma surgeons. The decision of which specialty should manage which injuries varies across different centers. Through these trauma chapters we will discuss what management decisions the majority of vascular surgeons should be comfortable managing as a part of a multidisciplinary trauma team.
Take a Listen
Check our debate between leading trauma and vascular surgeons about how to best develop a collaborative team to manage vascular trauma.
For relevant images and a more in depth discussion of this topic, please review Chapter 18: Abdominal Aortic Trauma, Iliac and Visceral Vessel Injuries(Aylwin and Jenkins 2022) in Dr. Rasmussen’s 4th Edition of Rich’s Vascular Trauma.
13.1 General Principles
As in all traumatic injuries, ensure that the patient is appropriately resuscitated with supportive care.
It is important to consider the broad principles and approach:
Urgency of situation
Resuscitation Efforts
Communication with Team
Optimal Exposure
Appropriate Equipment
Decision to maintain patency of a vessel vs. ligation is dependent upon the situation. During damage-control procedures where bleeding is not controlled and location of hemorrhage not known, the inclination is to ligate. The risk is organ ischemia, but the benefit would be patient survival.
Angiography can be utilized in conjunction to open operative explorations in areas of injury that are difficult to access/control (i.e. Zone 3 retroperitoneal hematomas)
Take a Look
Here is an image of the zones of the retroperitoneum, hosted by basicmedicalkey.com.
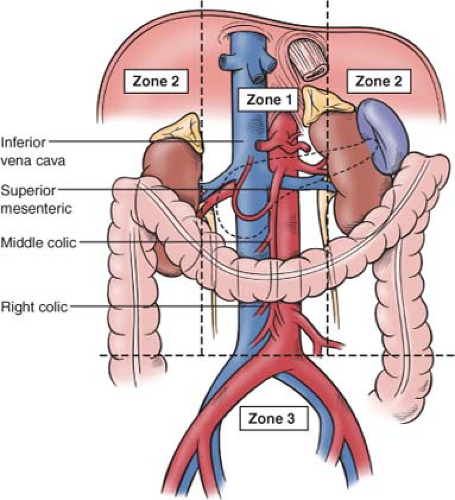{kind=link}
General Guidelines of Penetrating vs. Blunt Retroperitoneal Exploration
Zone I hematomas: explore whether penetrating or blunt mechanism.
Zone II hematomas: always explore if penetrating, do not explore during blunt unless expanding. Kidneys are in Zone II and are in the lateral gutters.
Zone III hematomas: always explore if penetrating, do not explore during blunt unless expanding.
13.2 Basic Exposure Techniques
Procedural Sequence in Operative Abdominal Trauma
Expose
Achieve Proximal Control
Explore and Evaluate Injury
Restore Flow
Supraceliac aortic and thoracic cross-clamping are important surgical maneuvers to control massive intra-abdominal bleeding in hemodynamically unstable patients.
Tips and Tricks
In order to get umbilical tape or vessel loop around aorta, use combination of Metzenbaum scissors and controlled pressure.
As you try to free the aorta from the connective tissue around it to get back to the spine, can use a metallic pediatric yankauer (small profile and blunt tip) as a dissection tool and push with the Metzenbaum scissors along with direct feel to get the aorta freed.
Can then use a right angle to get underneath the aorta.
Ensure that lumbar vessels are identified when trying to get around the aorta
“find the outside before you find the inside”
Can clip lumbar vessels with medium/large Weck clips
Use blue operative towels to cover and bring up the viscera to be held with the large retractors (i.e. Omni retractor) so your hands are free to operate.
Spine exposures with orthopedic and neurosurgical colleagues and transplant procurements are also a great opportunity to learn the tenets of rotating the viscera either right or left and exposing the retroperitoneum
Take a Listen
Check out our conversation with spine surgeons at HSS in New York City on collaborative work between vascular and spine surgeons to improve the safety of spine surgery.
13.2.1 Supraceliac Control
Supraceliac control is recommended prior to any medial visceral rotations if it is a Zone I hematoma.
Exposure
Basics
Exposure starts with midline laparotomy incision from xiphoid to pubis that may be extended to the first 2-3 cm of a sternotomy.
- This releases the inferior costal margins of the thoracic area under the diaphragm to pull the costal margins laterally and up – which suspends the patient’s rib cage up and away from the aorta and the abdominal contents
Recommend use of Omni retractor so that retractors can be placed under costal margin
Ensure that there is nasogastric tube placed by anesthesia
- Allows circumferential control of esophagus with either umbilical tape or penrose drain for appropriate left-sided retraction of the esophagus, away from the crus that is surrounding the aorta
Steps
Midline laparotomy incision supraxiphoid to pubis with release of costal margin (suspended away from abdominal contents)
Clear left lateral segment of liver by mobilizing left lateral segment either cephalad or tucked inferiorly to the right side.
For better exposure, place patient in reverse Trendelenburg to let the stomach down and pull it inferiorly to create a better window
- Esophagus is retracted to the patient’s left and the stomach pulled down (further retraction can be performed by a resident or operative assistant by putting their hand on the stomach and retracting it towards the pelvis)
Next, divide the crus overlying the aorta, using a large right angle and a bovie extender
Maintain adequate control during muscle dissection by feeling the aorta and its pulse (even a weak pulse)
Divide the crus over the aorta with electrocautery and with blunt dissection on either side.
Note: do not need to spend time to get circumferential control of the aorta like in an elective aneurysm repair.
Supraceliac aorta should now be exposed enough on either side to have a clamp appropriately placed to gain control
For more on exposure of the visceral aorta, check out Chapter 7
13.2.2 Visceral Rotation
Left medial visceral rotation (Mattox Maneuver)
Maneuver performed when aortic injury or a close branch off the aorta is suspected
Designed to give optimal exposure of the para-visceral segment of the aorta
The para-visceral segment of the aorta includes the supraceliac segment all the way down to the aortic bifurcation, primarily the left common iliac artery
Steps
Divide the white line of Toldt along the sigmoid colon and the left colon.
Establish plane in the retroperitonium
- Achieved through steady blunt dissection facilitated with Bovie electrocautery
The dissection plane is taken from the sigmoid/left colon up to divide the attachments ingrained in the spleen and the left kidney, then to the mid-line and then ultimately to the patient’s right.
Left kidney is almost always brought up
- It is generally easier and faster, because you do not have to take the time to find the plane above the left kidney
Take a Look
Check out this video for an example of a left medial visceral rotation by Dr. Alan Lumsden at Houston Methodist.
Right medial visceral rotation (Cattell-Braasch Maneuver)
Important when concerned about an IVC injury
Steps
Divide the white line of Toldt starting at the cecum and coming along the right colon.
Bring the cecum and right colon cephalad and then to the patient’s left.
- Note: it is actually not so much of a rotation to the midline and then the left, but bringing everything up cephalad and then left to the patient’s left costal margin — almost bringing the cecum and right colon up onto the patient’s left chest.
This plane is similar to the left medial visceral rotation as it is largely developed with blunt dissection in combination with Bovie electrocautery to open the retroperitoneum.
At this point, you will almost immediately see the left iliac vein and then the vena cava.
Continue to bring the left colon up until you see the right renal vein and kidney.
- At the superior extent, this will expose the head of the pancreas and duodenum.
Take a Look
Check out this video for an example of a right medial visceral rotation by Dr. Alan Lumsden at Houston Methodist.
13.2.3 Exposure of Infrarenal Aorta
The exposure of the infrarenal aorta is also called the transperitoneal inframesocolic exposure
Inframesocolic means that the transverse colon is reflected cephalad.
Steps
Hold up the transverse colon and drape it up cephalad to patient’s costal margin (can be held up with a blue towel and retractor).
Divide the ligament of Treitz (by the surgeon on the patient’s right) and get down to the fourth portion of the duodenum which should be to the left of patient’s midline.
Once divided, the left colon remains on the patient’s left and everything else goes to patient’s right.
- Note: this is not a medial visceral rotation because only the fourth portion of the duodenum and all of the small bowel is partitioned to patient’s right.
At this point, one should see the infrarenal aorta. The left renal vein is the most cephalad extent and the aortic bifurcation is the most caudal extent (located at root of colon mesentery).
The left renal vein can be ligated if necessary to facilitate aortic control
- Note: try to preserve the branches of the left renal vein that drain the left kidney (gonadal and lumbar) so that dividing the left renal vein is not as much of a detriment to the kidney
13.3 Management
13.3.1 Celiac Artery
Exposure
Origin of the celiac artery can be seen with left medial visceral rotation.
- This maneuver will expose the entire paravisceral segment of the aorta
Can also use anterior approach through the lesser sac (very similar to exposure needed for the supraceliac aortic exposure)
Stomach is retracted caudally towards the pelvis, lesser sac is opened, and then the stomach is pulled down further.
Pancreas is pulled down as well and the origin of the first centimeter of the celiac artery is now exposed.
Repair
- Small and proximal injuries to celiac - Primary repair may be an option use 4-0 or 5-0 prolene sutures.
Ligation
Large injuries with destruction of vessel wall - Primary repair may not be an option
Considered as damage-control situation to control bleeding and ligation considered as an initial step to save a patient’s life
Ligation may be tolerated if there is robust GDA collateral circulation. However, once bleeding is controlled, this should be assessed with doppler.
If the patient is stable or improving and particularly if there is clear signs of liver, pancreas or duodenal ischemia, then this should be reconstructed.
13.3.2 Common Hepatic Artery (CHA)
Exposure
Best visualized through that similar transperitoneal anterior approach for exposure of the celiac artery through the lesser sac.
Prior to identifying the common hepatic, you have to find the celiac and follow the branches
Recommend positioning in reverse Trendelenberg, the stomach inferior, and costal margins flared up to have the appropriate space
- This will expose the second and third portions of the celiac artery, and its major branches — including the common hepatic.
The common hepatic artery can not be visualized using left medial visceral rotation.
Repair
Primary repair is ideal
Ligation may be only option in damage control surgery
- If possible, ligation of the common hepatic proximal to the GDA is preferable as there will be retrograde flow from the GDA into the proper hepatic to maintain the viability of the duodenum, pancreas, and liver.
13.3.3 Gastroduodenal Artery (GDA)
Exposure
The gastroduodenal artery is the first branch off of the common hepatic artery and defines the junction between the common and proper hepatic arteries.
Repair
Primary repair should be sought if possible. If it is a damage control situation, then the GDA must be ligated to control hemorrhage.
Ligation
Assess patient’s condition, resuscitate, utilize the doppler, and assess the area distal to ligation to evaluate the consequences
If ligation showed appropriate collaterals, then the vessel can remain ligated
If there is clear ischemia, then there is a difficult decision between repair vs. shunt vs. permanent ligation
Consider metabolic consequences of ligation as well.
Decision is situationally dependent - the principles of damage control resuscitation and damage control surgery should always be maintained.
13.3.4 Splenic Artery
One of the key tenets of splenic injury is exposure. Ensure good retraction with incision up to xiphoid and alongside the left costal margin.
Low threshold for splenectomy for control of hemorrhage from the splenic artery or splenic parenchyma.
13.3.5 Superior Mesenteric Artery (SMA)
It is important to remember that a majority of these axial injuries are typically unsurvivable and proximal SMA repair is uncommon in the trauma setting. Even if the SMA is repaired and the bowel appears viable, it is preferred to delay abdominal closure and perform a second look 24-36 hours later or sooner depending on the patient’s condition.
SMA is divided into 3 segments based on its course
Segment 1: Aorta to Pancreas
Segment 2: Pancreas to Root of Mesentery
Segment 3: Mesentery to Small Bowel
Exposure
Visualization is dependent on the segment that needs to be exposed
Segment 1 (most proximal) - left medial visceral rotation.
Segment 2 (near head of pancreas)
Head of pancreas may need to be divided to get appropriate exposure
If distal to head of pancreas, can use inframesocolic approach
Segment 3 (most distal) - anterior transperitoneal approach
Repair
All efforts should be made to maintain flow through the SMA
Primary repair - performed on small injuries with 4-0 or 5-0 prolene suturing
Patchy angioplasty of interposition graft
For larger injuries
Conduit types: PTFE, Dacron, or autologous tissue such as proximal greater saphenous vein or deep femoral vein
Autologous vein is preferred in contaminated field, but can also use rifampin-soaked Dacron.
Tunneling is dependent on location, proximal segments would need 6-8 mm of graft while distal segments would need 3-4 mm.
Again, repair in a strictly traumatic setting is rare, because injuries that include the proximal mesenteric arteries are unlikely to be survivable. However, these techniques can be applied to other situations when assisting other surgeons who have to resect the SMA as a part of an oncologic resection or have induced an iatrogenic injury.
Take a Listen
Ligation
- Distal SMA segments may be more tolerant of ligation.
13.3.6 Inferior Mesenteric Artery (IMA)
IMA can be ligated in majority of cases.
Prior to ligation, assess the patency of the iliac vessels — specifically the internal iliac vessels.
If both celiac and SMA are patent, then the IMA ligation can be tolerated.
If there is concern for atherosclerotic disease or occlusion in the internal iliacs, then ligation may not be the preferred option and re-implantation may be considered.
For more discussion of evaluation and re-implantation of the IMA, see Section 10.3.2
13.3.7 Renal Arteries
Renal artery is unlikely to be reconstructed in a trauma setting (similar to SMA)
Most commonly, if there is an expanding hematoma in Zone II and the renal artery/parenchyma is damaged and confirmed as source of hemorrhage, a nephrectomy is warranted and there is no indication for repair.
In renal trauma, the renal artery is either not injured (with only injury to renal parenchyma) or renal artery is injured and thrombosed.
- If renal artery thrombosed, salvageability is unlikely due to prolonged warm ischemic time of the kidney.
Repair
Occurs if source of hemorrhage is from an injured renal artery that still has flow
- Seen during exploration of expanding hematoma in Zone II
Most commonly, if renal artery is injured it is ligated for damage-control
If patient hemodynamically stable, primary repair recommended
4-0, 5-0, or even 6-0 monofilament prolene suture
If a primary repair would compromise the lumen, then consider patch angioplasty
Distal branch artery injuries can be managed with endovascular coil embolization.
- Again, the decision to take the time to coil embolize is dependent on the patient’s current hemodynamics
Incidental CT findings
Types: intimal flap, fistula, and/or possible pseudoaneurysm of the renal artery
Management
The injury can be observed if there is continued renal perfusion and no flow limitation.
If it is a flow limiting injury with more than 50% stenosis caused by the intimal flap, it may be amenable to endovascular placement of bare metal stent to tack down the flap.