18 Venous Disease
Authors: Leanna Erete, Andrew Nickinson, Aminder Singh and Manj Gohel
18.1 Chronic Venous Insufficiency
18.1.1 Terminology and Presentation
What is chronic venous insufficiency and how common is it?
I thought the first question was going to be nice, easy and uncontroversial, but you’ve started with CVI. What you’ve highlighted is one of the main problems with venous disease, which is terminology. So if you type in chronic venous insufficiency into Google, you end up with, this enormous range of descriptions and how its used in lots of different ways, by lots of different people.
One of the problems is that this led to a lot of confusion among people within the venous space and everywhere else. A really important documents to guide people is the VEIN-TERM consensus document published in 2009.(Eklof et al. 2009) The lead author was Dr. Bo Eklof and this was a document where a group of venous experts around the world got together and said, okay, we need to be clear and define what all these different terms mean.
And one of the terms that was described was chronic venous insufficiency. The official definition is it is a venous disease between C3 and C6 on the CEAP classification. We’ll talk about that a bit later, I’m sure. But between C3 and C6. In practice, it is used to describe the entire spectrum of venous disease ranging from thread veins C1 all the way up to venous ulceration. But technically it is C3 to C6. And I would urge anybody who is learning about the terminology to look at the vein term documents.(Eklöf et al. 2004; Eklof et al. 2009)
And silly little things like great saphenous vein and small saphenous vein–I think UK is the only place where long saphenous is ever used and the real problem was LSV in lots of other countries will be the lesser saphenous vein, which is the small saphenous vein. So again, I’d urge anyone to look at that document.
How common is chronic venous insufficiency?
Chronic venous disease is very common, with the weather getting a bit nicer, people wearing shorts, you’re spotting, venous disease all over the place. The studies that have been done indicate that at least a quarter, probably up to a third of people have C2 to C6 disease. So a very common problem, with lots of people that need treatment.
The Edinburgh Vein Study found that half of the general population with chronic venous disease deteriorated over the 13 year study. Factors associated with disease progression included family/personal history of DVT. Of note, female gender, obesity, number of pregnancies, and smoking status were not associated with progression.(Lee et al. 2015)
Now we would like to discuss the classification and scoring systems, you mentioned CAEP, could you expand on that?
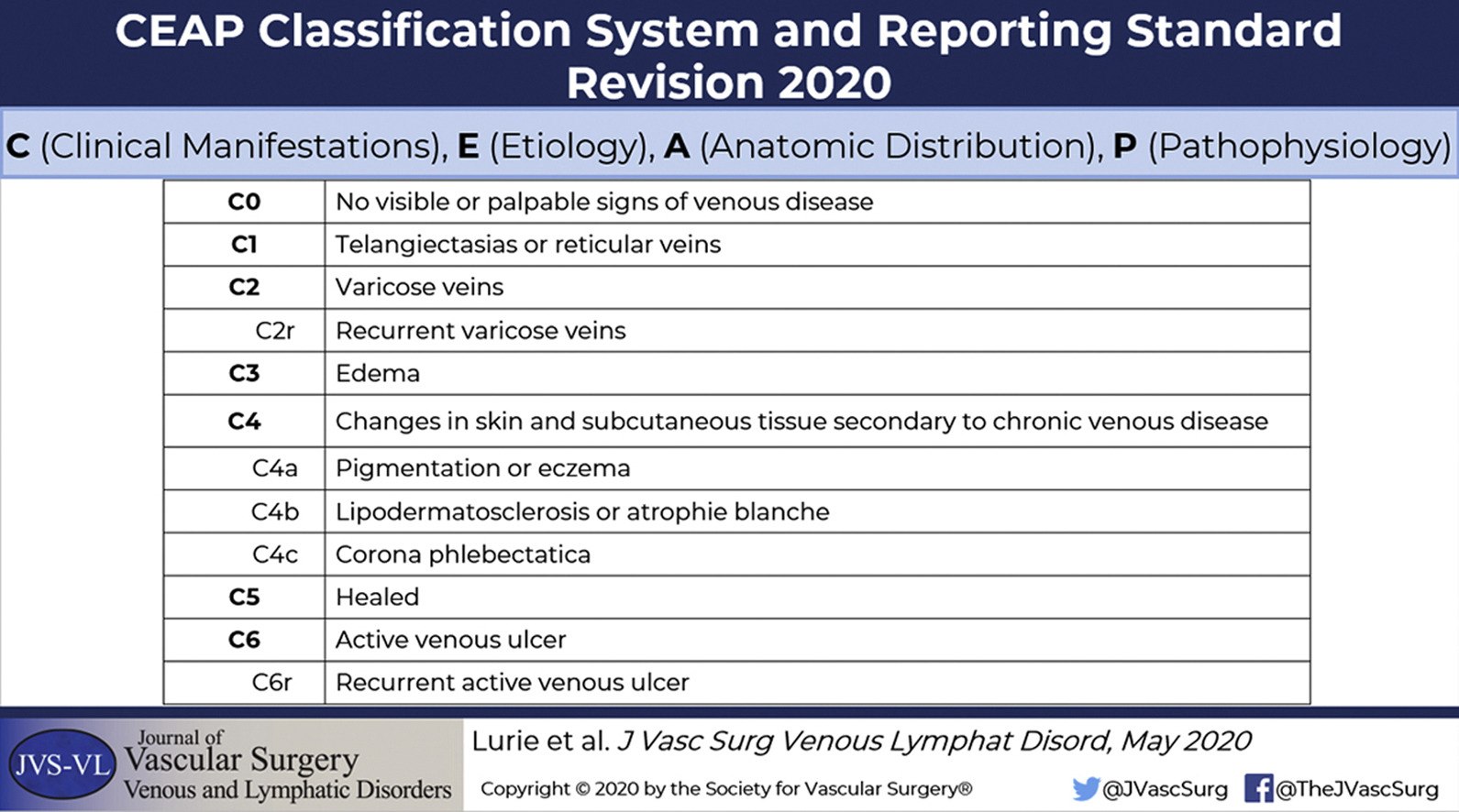
So CEAP–clinical, etiological (with an E because it’s American), anatomical, pathophysiological–classification system was introduced, I think in the mid 1990s, by the American Venous Forum. And it’s a classification system.
So if you have a patient that comes into your clinic with a venous problem, it’s a system to allow you to describe that patient’s current status in an objective, clear way. What it does not do is give you any information about prognostication and it isn’t useful for measuring responses to treatment.
So it is purely a descriptive classification system. And the most commonly used part is the clinical bit, which is C1 to C6. CEAP was just recently revised last year, a 25 year revision, which again, I would urge trainees to have a look at, Dr. Fedor Lurie was the lead author, and th is was a useful revision of CEAP.(Lurie et al. 2020)
Now in response to the limitations of CEAP, the Venous Clinical Severity Score (VCSS) was created. So this is a 10 item scoring system, each item scores between zero and three. So you get a maximum score of 30. Now this is designed to be responsive to treatment and complimentary to CEAP.(Vasquez et al. 2010)
There are lots of other things that have been described, quality of life tools or VDS, but I would say that those two (CEAP and VCSS) are the most relevant and important ones to know about. Many of the QOL tools are too cumbersome to use in day to day practice. We are in dire need of a easy to use clinical tool that is validated for assessment of patient reported outcomes. And again, the number of papers I’ve reviewed where people have reported CEAP scores as one of the outcome measures in response to treatments. That is not what it’s designed for, for example, you can never get lower than C5. You can never get better than a healed ulcer. So again, that’s the important distinction.
18.1.2 Evaluation
When we do see patients in clinic with chronic venous insufficiency, which type of imaging modalities should we use to investigate the function and the anatomy of the lower limbs?
If a patient comes to clinic, we can’t underestimate the importance of the clinical assessment. And when you assess these patients, you are really looking for the impact of their venous disease on their quality of life and the impact of the venous disease has on their normal function.
But also you’re looking for complications of venous disease. This is a clinical assessment. But then when ordering investigations, you really want to identify underlying treatable causes of their venous disease. And that’s the goal of any investigation.
Venous duplex imaging is obviously the first line, gold standard that pretty much anybody will go to around the world. And what that does is essentially gives you information about the venous flow, antegrade or retrograde or refluxing flow in superficial and deep veins.
It’ll give you information about the anatomy of the veins , which will help you to plan treatment, but it also gives you lots of other information as well. It gives you information in the common femoral vein, for example, if there’s good phasicity of flow or if there’s any scarring. It helps you to evaluate whether there might be some outflow obstruction, so duplex imaging is the absolute first line, gold standard. For more on venous duplex scanning, see Section 20.7.
Now, once you’ve done the duplex imaging, if there’s clinical suspicion, then of course we can move on to other investigations. So proximal CTV, MRV, venography, IVUS. But clinical assessments and duplex assessment are the bedrock of every assessment of every venous patient. So that’s the foundation.
18.1.3 Management
Moving on to the treatment of superficial disease. When we talk about treatment of superficial venous incompetence, I don’t think we can really get away from talking about the two major studies, the ESCHAR(Manjit S. Gohel et al. 2007) and the EVRA(Manjit S. Gohel et al. 2018) studies, which I know you’ve been involved with. Can you review what these studies showed and their importance in the care of our patients.
Before I go into the trials, I’m just going to go back a step and just talk about the general mindset that’s important for these patients. So what we’re treating with these patients is not superficial venous reflux. What we’re treating is chronic venous hypertension. So we’re treating a pathophysiological entity of which the superficial reflux is one correctable factor. And the reason that’s important is that there may be other correctable factors, such as venous outflow obstruction, which may be addressed. Decision making also takes into account patient presentation. For example a patient with asymptomatic varicose veins, even with proximal obstruction and superficial reflux, should still only be treated with compression.(Boezem et al. 2011; Wittens et al. 2015)
But there are also going to be lots of uncorrectable factors, such as poor mobility, heart failure, dependency, ankle stiffness. If your ankle is stiff, you can’t use your calf muscle to pump effectively. You don’t have that mechanism for reducing the venous pressure in your legs. So the success of these treatments, particularly for the ulcer population, has to be taken in the context of treating venous hypertension as well.
Having said that, the aim of these trials was really very simple. Most patients with venous ulceration have superficial reflux. So what is the role of treating the superficial reflux? That’s the simple question that was asked by these trials.
The ESCHAR trial recruited between 1999 and 2002, and included 500 patients with healed and open leg ulcers. They were either randomized to compression or compression and traditional, superficial venous surgery (stripping or ligation). And that trial was very clear. It showed that with venous stripping there wasn’t a benefit for healing, but there was a significant and sizable reduction in the risk of ulcer recurrence.(Manjit S. Gohel et al. 2007)
So one of the criticisms of ESCHAR was lots of people didn’t have the same surgery. Lots of people had just ligation alone, et cetera. We don’t really do stripping anymore, it’s all endovenous. So EVRA really aimed to bring the ESCHAR trial up to modern practice. We randomized 450 patients with open leg ulcers to early endovenous treatments, delivered within two weeks versus a more delayed approach. What EVRA showed, again is common sense, if you deal with the underlying problem (usually superficial reflux), the venous ulceration healed significantly quicker.(Manjit S. Gohel et al. 2018)
So putting them together, there is a clear, unequivocal argument for treating the superficial reflux in these patients as quickly as possible.
18.1.3.1 Endovenous
Can you broadly outline the different treatment options that can be offered to patients with superficial venous reflex?
I have counted about 42 different ways of destroying a saphenous vein. There are lots of different treatment options. Do something that you’re trained in and proficient with and something that’s appropriate. Thermal ablation is in the NICE guidance and in lots of other international guideline documents has been combined, whether it’s radiofrequency or laser. Although foam sclerotherapy therapy, when studied in randomized trials, has lower technical success rates and lower vein closure rates, the clinical success rates in terms of healing are just as good. This reduced effectiveness in closing the vein, doesn’t really seem to translate into a significant drop in clinical effectiveness after foam sclerotherapy.
So I think the most important thing is not necessarily what you use, it’s doing it quickly and delivering it to the people that need it. However, there are a few relative contraindications to GSV ablation.(Atasoy 2015; Gloviczki et al. 2011; Lowell S. Kabnick and Sadek 2019) These include:
GSV >12mm width raises concern for incomplete obliteration
Superficial GSV unlikely to be pushed down with tumescence - could cause staining or thermal injury to the skin
GSV tortuosity may limit the ability to pass a catheter and sufficiently ablate the vein
Acute superficial vein thrombosis.
Take a Listen
Check out our episode with Dr. Andrew Meltzer as he discusses some controversies in variations in practice regarding the use of endovenous ablation procedures in the United States.
When we are consenting patients for endovenous intervention, what risks should we discuss with the patient and that they need to be aware of?
You can spend an hour doing this, if you’re being very diligent. But what I say to patients are that there are generic risks of venous thromboembolism, as is the risk of any intervention. And I think that’s worthy of specific discussion after endovenous procedures, but I quote a risk of around one in 200 for most endovenous interventions. Extension of proximal thrombus into the deep system is termed endothermal heat-induced thrombosis (EHIT) and is evaluated and treated aggressively in the United States.(Sadek et al. 2013; Lowell S. Kabnick et al. 2021) EHIT is defined as:
| EHIT Grade | Description | Treatment |
|---|---|---|
| 1 | Extension to SFJ | None |
| 2 | Extension into deep system <50% of lumen diameter | Close observation vs anticoagulation |
| 3 | Extension into the deep system >50% of lumen diameter | Anticoagulation |
| 4 | Occlusion of the femoral or popliteal vein | Anticoagulation |
There’s always a risk of bruising. And if you do phlebectomies, what I often tell people is that bruising sometimes looks worse than it feels. And with the thermal interventions in particular, I think the risk of nerve related complications, so some numbness or some nerve pain, are worthy of mentioned, and of course the risk of recurrence. Recurrence of varicose veins in the lateral thigh may be related to untreated anterior accessory greater saphenous vein disease.(Laredo, Lee, and Neville 2010)
Foam sclerotherapy has a different mechanism of action. It’s a detergent that’s injected into the vein that destroys the endothelium. And there are some people that have associated foam sclerotherapy with some neurological events. So a very large registry that was organized by the manufacturers of STS recently looked at 10,000 patients in the UK and found very few events-around one in 4-5,000.
There are a number of complications related to sclerotherapy that should be understood. Hyperpigmentation is probably the most common complication (11-80%), but only a small percentage persist up to a year (1-2%). Incision and drainage of the thrombus 2-4 weeks after treatment may reduce hyperpigmentation. New appearance of fine red telangiectasias (AKA telangiectatic matting) is related to underlying vessel injury in 5-57% of patients and can persist up to 1 year (1%). Cutaneous necrosis is rare (<1%) and results from extravasation of sclerosing agent, injection into dermal arteriole, reactive vasospasm or excessive cutaneous pressure. DVT and cutaneous nerve injury are also rare.(Bergan, Pascarella, and Mekenas 2006; Munavalli and Weiss 2007)
Some people say that if there is a history of migraine, then the risk of these neurological events might be a little bit higher. So, a little bit of caution, although in practice, I’ve treated many people with migraines. But if you believe the literature, one in four or five, people have got a little ASD and obviously we treated lots of those people, so the risks are very low but it’s just important to have that discussion beforehand.
Are there any techniques that we can use to mitigate some of these risks?
So I think VTE is something that is really worth specifically discussing. It’s a very rare event after superficial venous interventions, but it’s potentially catastrophic, with sometimes national press coverage for bad outcomes. What we’ve got to realize is that the rate of VTE events is very low, there are almost certainly some people that have a higher risk. And so what we’ve got to get slightly smarter about is identifying the people that have a higher risk of VTE and maybe giving them prolonged course of thromboprophylaxis, as well as appropriate counseling and mitigation as well.
So it’s about getting smarter about risk assessment. The current risk assessment tools are not really fit for purpose when it comes to superficial venous intervention. So the department of health or the Caprini tools don’t really take into account some of the really important factors that I think do impact on VTE risk after superficial venous interventions.
There’s nothing validated, there’s nothing widely available, but we have a local, specific risk assessment for patients having superficial venous interventions. There are major risk factors we look out for, such as previous ipsilateral VTE, active malignancy, but also significant chronic inflammatory conditions (i.e. inflammatory bowel disease), these patients have a much higher risk of VTE than we previously recognized. There are also minor factors, superficial vein thrombosis, obesity, comorbidities. All of these things are put together and we come out with a score. For patients above a certain threshold, they get offered extended rivaroxaban or low molecular weight heparin.
In addition, it is important to implement mitigation. So traditionally things like a contraceptive pill, HRT and Tamoxifen, we wouldn’t usually stop them for a local anesthetic procedure, but being on an estrogen containing pill doubles or triples your risk of VTE. It’s an easily reversible thing in the short term that can be done. So for my patients, I would normally recommend that we stop the pill or HRT a full month before and after the procedure.
For preventing EHIT specifically, the radiofrequency ablation (RFA) catheter should be placed 2cm from the SFJ. EHIT is a primarily technical complication.(Joh et al. 2014)
You mentioned it an extended course of anticoagulation for those patients with risk factors. Is there a specific timescale locally that you use for this?
The venous forum produced some guidance the year before last in exactly this area. We often only do about a week or 10 days for a lot of these patients. However, if there’s an ongoing, persistent risk factor, then actually the VTE risk persists for four to six weeks, and thus there may be an argument for up to six weeks of therapy in particularly high risk patients.
However, if they are really that high risk, you’ve really got to question whether a superficial venous intervention is needed, balancing the risks and the benefits. But since for some patients the high risk period persists for at least another six weeks afterwards, be careful not to stop prophylaxis too soon.
Moving on to a more specific question about treatment, what is the role for treating and incompetent perforator veins in these patients?
In general, the more advanced the venous disease, the more likely it is that the disease is recurrent, the more likely there is to be deep venous disease or posts thrombotic disease, and the more likely you are to finding incompetent perforators. If you imagine these patients with venous ulcer, it is very common to find perforators, and if you take a sort of super aggressive role saying you’ve got to obliterate every single bit of reflux you can find, then you’d be doing a couple of perforators in every single patient, and that is the approach of a number of centers around the world.
The pragmatic reality is, number one, if you ablate the superficial reflux, we know that a lot of these perforators actually become competent because we’ve got rid of the outflow or you’ve changed the dynamics in some other way, and they’ve become competent. Number two, even if they’ve stayed incompetent, the clinical benefit is still there and is usually still pretty durable. The clinical criteria most often used to as an indication for treatment is >350ms of deep to superficial reflux, diameter greater than 3.5mm (associated with reflux in 90% of patients)(Sandri et al. 1999) and near a healed or active ulcer.(O’Donnell et al. 2014; Min, Khilnani, and Golia 2003; Rueda et al. 2013)
Now, of course, there may be some people that develop recurrent problems and then there can be a more targeted approach to the perforator. The ESCHAR and EVRA studies did not target perforators at all and the outcomes in the EVRA study was the best healing rate of any published prospective leg ulcer study. So, putting all that together, it’s difficult to make a case for aggressive treatment of perforators first up. Having said that for some people with recurrent disease, it’s not uncommon to have a big mid thigh Huntarian perforator or Cocker’s perforator lower down on the medial calf. So, I do treat perforators, but almost always it’s in recurrent disease with recurrence or deteriorating symptoms.
18.1.3.2 Open Surgery
So we’ve discussed quite a bit about endovenous intervention. Is there a role for open surgery in some patients?
Open surgery remains the most commonly used superficial venous intervention around the world, and there are still lots of centers in the UK that primarily offer open surgery. Being balanced, it’s a very effective treatment if you do it well and if you use modern approaches, such as tumescent anesthesia and ultrasound guidance, then actually some of the traditional issues with open surgery, which are often technical and complication related, don’t really apply.
Having said that, all the randomized trials have shown the same thing while the effectiveness may be as good in open surgery done well, the recovery is much better after endovenous ablation. So it’s difficult to make the case for open surgery when you’ve got something that is so well established and the complications just so low, and it’s cheaper when you look at their theater capacity, et cetera.
So, I think there has to be a move towards endovenous, but there are lots of things stopping this. In Germany, for example, the reimbursement is greatest for open surgery. So surprise, surprise, there are still lots and lots of open varicose vein operations. For trainees, it is important to recognize that if you want to change practice, the single biggest driver for change is reimbursement. You can change whatever you like. So, I’ve treated maybe three patients with open surgery in the last five years. One was a GP, who I had treated the other leg with open surgery a few years earlier, and she said, “I want the same operation, please.” So I did struggle to argue with that. The other two were big three, four, five centimeters saphenovarices in the groin. So specific indications, but not really for most patients.
For deep venous reflux, surgical management follows a relatively complex algorithm.(O’Donnell et al. 2014) Valve prolapse due to vein wall dilation may be treated with external banding. Isolated valve prolapse may be treated with external valvuloplasty, and in severe cases an internal valvuloplasty. When no adequate valve exists, then valve transplant from a distant source, such as the axilla, may be necessary.(Kabbani et al. 2011) These are not commonly performed procedures and should be referred to centers with significant experience.
18.1.3.3 Medical Management
So we’ve talked about endovenous and surgical treatment, but are there any pharmacological therapies that can be used in patients with chronic venous insufficiency?
So we’re pretty skeptical in the UK, when it comes to venoactive or pharmacological treatments. If you go to Europe, they love them. They’re over the counter in a lot of pharmacies. The drug with probably the most evidence is something called Daflon, micronized purified flavonoid fraction.
So flavonoids are naturally occurring, venoactive compounds. There are a whole variety of effects, only some of which we understand. But a lot of studies have shown improvements in edema and heaviness. Daflon is marketed by a French company and it’s got good evidence, but they do not see places like the UK as a big enough market because of our inherent skepticism over these sort of things, to make it worth their while to go through the marketing and the regulatory processes. So it’s not available. But patients that have gone to France and picked it up over the counter and have said it works well. So there may be a roll for some venoactive medications such as pentoxyphyllin —there’s some good evidence that it accelerates healing of leg ulcers.
But I don’t think we’re very receptive in the UK in general, not in the vascular surgery community to prescribe pharmacological or herbal type remedies.
Wound management in patients with venous insufficiency however has many medical adjuncts.Topical agents include excimer (cadexomer) iodine, silver sulfadiazine, silver-containing dressings, growth factors or cell-based therapy.
What are the healthcare costs associated with the lower extremity venous disease?
The educated guesstimates in the UK, NHS, is around 2 billion pounds a year. The UK NHS budget is about a 120 billion. So, up to about 2% of the budget, and that’s just C6 disease. We’re not even going into all of the other diseases, the associated cellulitis, but also not only the healthcare costs, but the societal costs, the time off work, the other things. And then of course the superficial vein thrombosis, VTE and other associated diseases, it’s a massive underestimate.
18.1.4 Other Complications of Superficial Venous Disease
18.1.4.1 Superficial Vein Thrombosis
You mentioned superficial vein thrombosis, also known as superficial thrombophlebitis. What is it and how do you manage it?
I’m very pleased you used both terms because I’m going to take the opportunity to encourage robustly the use of superficial vein thrombosis rather than thrombophlebitis. The problem with thrombophlebitis is it is too closely associated with an infectious etiology, which can lead to useless courses of antibiotics. Of course, there’s no infection, it’s a thrombus in a superficial vein. Traditionally, it’s just been seen as just a bit of a nuisance and let’s not worry about it, treat with analgesia and anti-inflammatories, and you’ll be fine.
It can be a really sinister pathology and associated with VTE. If you think of how many thousands, millions of people that have varicose veins. They don’t all get clots in their varicose veins. They’ve all got stasis to a certain extent but they don’t get clots. So it’s more than just the flow dynamics going on here. These people likely have an thrombogenic innate tendency that leads to this. That’s shown out in the studies, some really good work in some French studies, such as the POST study. They identified patients who were scanned with superficial vein thrombosis, and a quarter of them on their first duplex scan had a DVT. A lot of these DVTs were remote to the superficial vein thrombosis.(Decousus et al. 2010) So they’re not all extending into the deep vein—they were remote—confirming this idea that actually a thrombogenic problem is going on here. A patient with superficial vein thrombus and a previous history of DVT could suggest a subsequent risk of VTE up to 20%.
So in the latest ESVS guidelines, there is quite a lot of content about SVT treatment with algorithms. I would urge people to have a look at that, and it’s important to risk stratify people. Limited disease can be followed with ultrasound at 1-2 weeks, but the closer you are to the junction, the higher VTE risk, and actually for anyone other than just a bit of clot in a varicosity, anticoagulation is the treatment of choice to reduce progression to VTE.(Kakkos et al. 2021; Di Nisio, Wichers, and Middeldorp 2018; Scovell, Ergul, and Conrad 2018)
| NSAIDs and Warm Compresses | Anticoagulation |
|---|---|
| Low risk Patients | High risk patients |
| Segment less than 5cm | Segment greater than 5cm |
| Remote from SFJ | Less than 5cm from SFJ |
CALISTO is the largest RCT and used treatment with 2.5mg SC Fondaparinux.(Group et al. 2010; Blondon et al. 2012) Rivaroxaban did subsequently demonstrate non-inferiority.(Werth et al. 2016) So look at the guidelines, it’s very clear what we should be doing with these people, evidence-based, Once the anticoagulation is done, they need to be re-scanned and that residual incompetent, scarred thrombogenic, saphenous vein needs to be ablated or excised, otherwise they’ll recur. So a real change in mindset and level of aggression.(Kakkos et al. 2021; Di Nisio, Wichers, and Middeldorp 2018; Scovell, Ergul, and Conrad 2018)
Pregnant patients are often high risk for lower extremity venous complications and pose difficult clinical challenges. Extensive superficial vein thrombus in pregnant patients should be treated with LMWH and paused at delivery.(Kupelian and Huda 2007; Litzendorf and Satiani 2011) If symptoms persist 3-6mo after delivery, the further workup for pelvic congestive syndrome may be required with a transvaginal ultrasound or cross sectional imaging.(Labropoulos et al. 2017)
18.1.4.2 Bleeding
What’s your approach to managing patients with bleeding varicose veins?
Really important question. It is a vascular emergency. There are several depressing reports of patients having died from bleeding from a varicosity. These are often elderly patients who are frail, with limited mobility , and therefore can’t bend down to press on the bleeding varicosity down by the ankle ulcer. There’s some very grim photos in various case reports and it’s really sad. There’s two or three photos that I’ve seen where an elderly patient has not wanted to wake their partner and so has gone and laid down in the bath with this bleeding vein that they couldn’t control and basically exsanguinated.
So, it’s a vascular emergency and these patients should be seen and assessed and their superficial venous disease should be dealt with as soon as possible. We have an emergency clinic running and anyone with bleeding veins have the same urgency as the CLI patients and they were treated there and then.
In terms of the treatment, there’s two aspects: you want to decompress the venous hypertension by ablating the saphenous reflux, but for the specific bleeding area, I think there’s a real case for some local foam sclerotherapy. You want to block off that vulnerable bleeding vein to ensure that this doesn’t happen again. But again, if anyone receives a referral, these are people to see straight away.
18.2 Acute Deep Venous Thrombosis (DVT)
So let’s move on to discuss deep venous thrombosis. You’re recently involved in the European society of vascular surgery, venous thrombosis guidelines. In the most part, calf DVTs are managed by medical teams or dedicated DVT services within the hospital. So in this section, we’ll be focusing mostly on proximal DVT.
18.2.1 Demographics
18.2.1.1 Physiology
In medical school, we’ve learned a lot about Virchow’s triad and the etiology of venous thrombosis. Does that simple concept still hold true today?
I think it does. There’s a few caveats and a few nuances, but I think the principle that the flow, the vessel wall, and the blood constituents are the main factors that affect whether or not you get thrombosis in a vein is still pretty solid. However, there is also a real change in mindset about the whole idea of provoked and unprovoked DVT. Again, I would urge people to look at some of the new areas that we’ve covered in these guidelines.
18.2.1.2 Prevalence
Incidence of DVT increases with age by a factor of 1.9 per 10 years. Of patients who develop DVT, 1% will have phlegmasia and 10% may develop a pulmonary embolism.
For post-thrombotic syndrome, 17% will develop at 1 year and 29% by 8 years after the initial DVT. For recurrence, 30% will develop over 10 years but the highest risk for recurrence is in the first year.(Beckman et al. 2010; Bulger, Jacobs, and Patel 2004; Meissner et al. 2007)
18.2.1.3 Etiology
You mentioned there about potential risk factors for DVT, and that can be classified into these provoked, which can be transient or persistent, and then unprovoked risk factors. Can you talk about some of the specific factors and causes?
In general, what’s been happening for several years is a recognition that there are some DVTs that happened with a clear provoking factor—a common major, transient, provoking factor is major surgery, for example. So a lot of DVT are caused with that clear provoking factor, but there’s an enormous population of people that don’t have a clear provoking factor at all, or have a minor factor that may or may not have contributed.
So traditionally there’s been a dichotomy between provoked and unprovoked. If it’s provoked, they get a limited period of anticoagulation is unprovoked it’s long-term anticoagulation. And certainly the last big thrombosis guidelines was the ACCP guidelines, the American CHEST guidelines, and that’s what they suggested, but it’s much more nuanced than that.
What we’ve got to remember is that there are some provoked DVTs where there’s much higher risk, and those are there’s some unprovoked DVTs, which actually there may be other factors that you need to take into account. So I think for those people that are interested in this area, it’s really important to get to the nitty-gritty. So, long-winded way of answering your question. But here are some risk factors:
Major provokes
Surgery
Major trauma
Minor provoked
Shorter periods of immobility - a few days sick in bed with the flu
Contraceptive pill - depending on whether it was just started or the patient has been taking for two to three years
In the guideline document is a big, long list of other things where for people to think about it and consider.
In this review we are discussing mostly lower extremity DVTs, however catheter-associated DVTs are sometimes encountered on examinations. In general the DVT is considered to be a result of the line. However, management is treatment of the DVT with or without line removal. If the line is functioning well and the patient requires the line for other therapy, then simply treating the DVT with anticoagulation should be sufficient.(Kearon et al. 2016; Kovacs et al. 2007) Treatment is similar in patients with cancer.(Debourdeau et al. 2009)
Prevention is a key component to mitigating the impacts of DVT. One of the more common risk stratification tools in the United States is the Caprini risk assessment model.(Bahl et al. 2010) Patients identified to be high risk according to the Caprini risk index require mechanical prophylaxis, pharmacological prophylaxis and early ambulation.(Gould et al. 2012; Laryea and Champagne 2013)
In those patients where, after you’ve taken a thorough history, there’s no obvious provoking factors. Is there a role for screening for occult malignancies and thrombophilias?
For thrombophilia testing, the history of it is really interesting. When they were first identified and our ability to screen them first became available, there’s a lot of excitement because people thought they were going to be able to identify a clear cause for all of these unprovoked DVTs. The reality is that at least 50% of them, there’s no identifiable thrombophilia. So what it almost certainly means is there’s lots of thrombophilias that we haven’t yet identified, we can’t test for. So it hasn’t really been the panacea in that regard. The other pragmatic reality for the thrombophilias is that if we’re going to be putting people on long-term anticoagulation anyway, the additional value of testing for these things is really very minimal.
And the ones that are really important—the thrombosis history is so stark that they normally smack you in the face. So I think it’s generally gone out of fashion. And again, there’s only very specific circumstances where we would suggest testing them:
If you’re going to be trying to stop anticoagulation, for some reason, the patients don’t want to be on it, or if there’s bleeding risks
There’s a clear family history. Then it might be worth excluding some of the more sinister thrombophilias.
Otherwise, certainly not a role for routine testing and similarly for malignancy—for unprovoked DVT, the prevalence of an underlying malignancy is somewhere between 6-10%. The studies that have looked at an aggressive, thorough assessment process rather than a more selective process, have picked up a few more cancers, but the additional cost in terms of anxiety, additional investigations, et cetera, and no demonstrable improvement in outcome has meant that the guidelines have not recommended routine cancer screening beyond the appropriate, symptom driven age and sex specific screening—PSA, breast assessments, colonoscopy, etc.
One unique situation is recurrent or migratory superficial vein thrombosis, particularly in older patients, can be associated with an underlying malignancy.(Litzendorf and Satiani 2011)
For patients with established diagnosis of thrombophilia (Factor V Leiden homozygous mutation, antithrombin deficiency, prothrombin G20201A homozygous) who become pregnant, recommendations state they should be on LMWH prophylaxis during pregnancy and 6w postpartum regardless of personal history of DVT.(Heit et al. 2005)
18.2.2 Evaluation
What is the algorithm for investigation?
The most important part is the first component of the algorithm, which is an assessment of the pre-test probability of DVT. So anyone who comes with a DVT, you can go through a validated tool. The most common is the Wells probability score, which is a series of questions and give you an indication as to whether a DVT is likely or unlikely. (Tritschler et al. 2018)
If a DVT is likely, then the algorithm is to do a scan, very straightforward. If a DVT is unlikely, then the algorithm is to do a D-dimer. Because if that is negative, DVT is effectively excluded. The guidelines are very clear on the assessment process, but a lot of this won’t reach our radars as vascular specialists at all until the DVT has been diagnosed, so we don’t appreciate the importance of the early stages. So again, a quick plug for the guidelines, there’s a very nice algorithm, beautiful colors—I definitely recommend having a look.
On ultrasound, acute DVT is characterized by an enlarged vein with a non-compressible lumen and hypoechoic thrombus. Chronic post-thrombotic scarring is often contracted with echogenic appearance.(Yusof et al. 2019) For more details, see Section 20.7.
18.2.3 Management
18.2.3.1 Medical
So the exact choice and duration of anticoagulation in the management of a DVT is probably beyond the scope of this podcast, but on the whole are DOACs preferred over vitamin K antagonists, such as Warfarin and why?
In a word, yes, lots and lots of studies, funded by big companies that make DOACs, have been done and they’ve all shown fairly consistent things. They’ve shown that the DOACs are as effective as the vitamin K antagonists at preventing DVT. They have almost always a significantly lower bleeding risk, but they’ve got this enormous added convenience of not needing regular blood tests, not having this dietary limitations, and the erratic control, et cetera. So the general direction of travel is inexorably towards more and more use of DOACs.
A couple of other areas where DOACs have really shined: The tendency is to recommend longer courses of anticoagulation and often indefinite anticoagulation. A number of studies, both rivaroxaban and Apixaban have looked at the effect of a lower dose of DOAC in these patients. So if you need to extend anticoagulation, can you use a lower dose, a prophylactic dose, so 10mg of rivaroxaban or 2.5mg BID of Apixaban. The results have been impressive because the prevention of recurrent VTE is very good, the same as the therapeutic dose, but the bleeding risk is much lower. So you’ve got this additional benefit of being able to give an even load those with even lower bleeding risk.
And the real icing on the cake for the DOAC has been a few recent studies that have been looking at cancer patients. Traditionally cancer patients where low-molecular weight heparin only, not for DOACs.(Kearon et al. 2016) But the Hokusai study(Raskob et al. 2018) and the Caravaggio study(Agnelli et al. 2020) more recently have both looked at Edoxaban and Apixaban in the context of cancer and have shown that actually they’re very effective. In addition, a recent meta-analysis found that recurrence rates were lower with DOACs, but bleeding rates were no different.(Dong et al. 2019; Rossel et al. 2019)
In almost all of the areas, DOACs are demonstrating their superiority. The one very notable exception is antiphospholipid syndrome, particularly triple positive antiphospholipid syndrome. This is a pretty nasty acquired thrombophilia where Warfarin is still the gold standard.(Pengo et al. 2018)
To step back a little, trainees should make sure they understand some basics behind the coagulation pathway and anticoagulants. Warfarin is one of the most studied and longest used anticoagulants and is a Vitamin K antagonist. Vit K is essential for activation of factors IX, X, VII, prothrombin (II), C and S, which are integral to the extrinsic pathway of coagulation.(Fair, Marlar, and Levin 1986; Wu, Morris, and Stafford 1991) The extrinsic pathway is activated by vessel wall damage and exposure of tissue thromboplastin or tissue factor (TF), which binds Factor VIIa activating Factor X and Xa.(Morrissey 2001)
Warfarin induced skin necrosis is important to understand, although very rare (0.01-0.1%). This occurs shortly after initiating warfarin and presents with purple, cool, painful toes and punctate areas of necrosis and petechiae. Treatment includes immediate cessation of warfarin and transition to LMWH, normalization of INR with Vit K and FFP.(Pourdeyhimi and Bullard 2014; Tran et al. 2013)
Reversal agents are also another tested topic in the medical management of vascular disease. Other anticoagulants and their reversal agents include:
Dabigitran - Idarucizumab.(Glund et al. 2019)
Edoxaban, apixiban and rivaroxaban - andexanet alfa.(Connolly et al. 2019)
Nonspecific with some effect on other DOACs - PPC, Factor 7, and activated PPC.(Cuker et al. 2019; Kearon et al. 2016)
Finally it is also good to be aware of a few additional coagulation factors and their function:
Integrin glycoprotein GPIa/IIa - platelet aggregation
Protease-activated receptors (PARs) - platelet aggregation
Thrombomodulin - activation of protein C
Plasminogen activator inhibitor-1 - suppression of plasmin formation/fibrinolysis.
Patients with a proximal DVT, in the iliofemoral or the femoropopliteal segment, is there a role for elastic compression in the acute phase?
Traditionally people have been a bit nervous about putting compression on patients with acute DVT, concerns about causing propagation and causing PEs. A very important study was the ideal DVT study(Ten Cate-Hoek et al. 2018), run by Dutch colleagues, and a number of other additional studies more recently that have built on the original IDEAL DVT study.(Schreurs et al. 2022)
The short answer to your question is that early compression is really important. It’s a really positive thing to do within 24 hours and it’s proper compression. It’s not just the Ted stocking and see what happens. It’s 30 to 40 mmHg, so that in practice is a class two stocking with a bandage on top. The benefits are that this reduces the early pain and swelling of the DVT, but also interestingly, it reduces the risk of post-thrombotic syndrome and post-thrombotic venous obstruction. So if you put compression on early, it reduces the risk of them developing post-thrombotic syndrome. So a lot of focus has been on clearing the vein and early thrombus removal and thrombolysis and thrombectomy and all this sort of aggressive stuff. But just by doing the compression, we can have at least part of the same effect and we’ve just not been doing it. Very rarely do these patients get proper compression.
So there is a big section in the ESVS guidelines about the role of compression and algorithm as to when, how to use it, and how long do you use it for. What we want to see now is the DVT pathways around the country, around the world, updated and amended with this latest guidance.(Kakkos et al. 2021)
18.2.3.1.1 Complications - Pulmonary Embolism
More and more vascular surgeons are becoming involved with Pulmonary Embolism Response Teams (PERT) and so surgeons should be familiar with the acute management of DVTs that progress to pulmonary embolism. The majority of pulmonary embolisms simply require anticoagulation.
However, if a patient becomes hemodynamically unstable, such as develops hypotension, then the patient should undergo systemic thrombolysis.(Kearon et al. 2016) Contraindications to systemic thrombolysis include:
Age >75
Intracranial neoplasm
Intracranial/spinal surgery or trauma with the last 2 months
History of hemorrhagic stroke
Active bleeding or known bleeding disorder
Non-hemorrhagic stroke within the past 3 months.
Patients who do not immediately respond to systemic thrombolysis, are a high risk of bleeding, or in shock that may cause death before thrombolytics take effect, then catheter based thrombus removal may be considered. This complex decision making is best made through the previously mentioned PERT.(Xenos et al. 2019) Endovascular techniques include:
Thrombus fragmentation
Suction thrombectomy
Rotational embolectomy
Ultrasound assisted thrombolysis
There are very high risk procedures and complications include pulmonary artery perforation, pericardial tamponade, cardiogenic shock, hemaglobinuria or other hemorrhagic complications.
18.2.3.1.2 Complications - Post Thrombotic Syndrome
One of the concerning complications of a DVT, particularly a proximal DVT is post-thrombotic syndrome (PTS). Can you recap the symptoms of PTS and how it’s diagnosed?
PTS is a fairly amorphous entity that includes a series of patient symptoms and clinical signs that develop after deep vein thrombosis. That’s deliberately very vague, because the condition is so variable. In terms of diagnosing PTS, the official diagnostic tool is a score of five or more on the Villalta scale. The Villalta score is another one of these tools that have been developed for both making a diagnosis, but also assessing progression of PTS.(Kahn et al. 2014; Villalta et al. 1994)
But in terms of sort of symptoms—people get swelling, heaviness, pain. There is a very unique symptom, which is venous claudication, which is almost pathonogmonic of post-thrombotic syndrome with venous outflow obstruction. It’s this pain which has a bursting tense quality in the calf on exertion, which does settle on stopping, but it takes a lot longer than arterial claudication. So sometimes people will take half an hour to get better and the leg has to be elevated. So that’s venous claudication and that’s often the most disabling symptom. But of course, people can develop the same clinical complications than you can with any venous disease—skin changes, lipodermatosclerosis, venous leg ulceration, et cetera. Those are the summery of symptoms for PTS, seen in up to 50% but probably closer to 25% of proximal DVT.
18.2.3.1.3 Complications - IVC Filters
A quick question about IVC filters. As vascular surgeons, we sometimes get asked about the appropriateness of inserting an IVC filter. When would you consider one and how long can one stay in situ for?
So short answer is I virtually never consider one, and if already in situ, remove as soon as possible. Let’s expand on this a little bit. So the history of IVC filters is a painful story, particularly in the US, super aggressive use of IVC filters, very few of them retrieved, lots of IVC occlusions, and major lawsuits against big companies. The most important factor in successful IVC filter retrieval is dwell time less than 7 months. Type of filter, tilting or protruding struts are not associated with failure. Adverse events have found to be as high as 2%.(Desai et al. 2017) That’s led to a worldwide, reluctance to use IVC filter, so now we may not be using them in some cases when we should be using them. The traditional indications and reasons for using IVC filters included weird and wonderful things like floating thrombus and other factors.
The reality is the only real indication that we could come up with was when there’s a proximal DVT, and there’s a clear contraindication to anticoagulation. So if there’s no anticoagulation, then the risk of propagation and PE is reasonably high, so there is a strong case for a temporary IVC filter. If a patient is anticoagulated, very rarely can the case be made for an IVC filter. I don’t want to go into nuanced details—such as where somebody already had a PE there’s right heart strain, there may be some anatomical features that you’re worried about, their anticoagulant control is borderline—there might be specific cases, but this is really very rare. Most people anticoagulated do not need an IVC filter.
A rather challenging and unique patient would be a pregnant patient with a DVT and placenta previa. Anticoagulation is contraindicated in placenta previa and in addition, an infrarenal IVC filter is also contraindicated, so she would require a suprarenal IVC filter.(Bates et al. 2018; DeYoung and Minocha 2016; Harris, Velineni, and Davies 2016)
In the setting of a thrombosed filter, a patient may require urgent intervention if they develop phlegmasia. Suprarenal filter placement may be useful during the procedure to prevent embolization. Removal of the IVC filter is contraindicated unless all clot is cleared.(Sheth et al. 2015; Teter et al. 2019)
18.2.3.2 Surgery
So clot burden reduction techniques are a hot topic at the moment. Before we talk about endovenous techniques, is there a role for surgical venous thrombectomy? And when would you consider this?
Open thrombectomy is part of the spectrum of early thrombus removal techniques. It used to be very popular, a very satisfying technique—I think I’ve done it three times. They’ve all been for the same sort of indication, which is phlegmasia, severe limb threatening post DVT change, and in a patient where they weren’t candidates for thrombolysis. However, if you’re with a patient where the leg is threatened, you can’t anticoagulate them, you can’t thrombolize them. Then in that case this is a sort of last ditch approach. But if that’s not the case, then almost always a catheter based approach is less invasive and more acceptable.
In addition, most people have got more training. Trainees should read some of the descriptions of open thrombectomy— it’s a very satisfying technique, but it’s quite involved. It involves finding and exposing the common femoral, deep femoral and femoral veins, applying tight compression around the lower leg to milk the clots out distally to proximally. So the original descriptions are really interesting, but really very rarely would we need to do that.(Comerota and Aziz 2019)
18.2.3.3 Endovascular
So you’ve mentioned catheter directed techniques for clot burden reduction. Some recent trials have challenged our thinking on the appropriateness of these techniques, such as the ATTRACT and the CaVent trial. What’s your take on the current evidence?
This is very controversial. The fundamental issue here is that the trials that have been done almost certainly would not have included a large number of people who would benefit from interventions in the opinion of the investigators. So if somebody has got severe DVT, it is unlikely, particularly in the US, where the ATTRACT trial was done, but these people would have been randomized into the trial.
So the immediate criticism of the trials is that this is not reflective of the population. You’ve excluded the people that benefit, so it’s an underestimate of the benefit of the technique. But if we look at trial results ourselves, there is a modest benefit. In the CaVent trial, PTS rate was reduced. The quality of life was less impressive, but the PTS rate was reduced moderately.(Haig et al. 2016) And in the ATTRACT trial, when they subgroup analyzed the iliofemoral DVT group, then there was a reduction in the number of people who develop moderate and severe PTS. So I think the numbers are something along the lines of, you’d have to treat 10 people with thrombus removal to prevent one person developing moderate to severe PTS.(Vedantham et al. 2017)
So then the discussion is are those numbers needed to treat appropriate for intervention? Particularly when you then start to consider the additional need for stenting and long-term surveillance, et cetera. So I think the jury is very much out. You’ve got really stark, strong, firmly held unshiftable views on both sides of the argument and what we need is a bit of nuance. What we need is everyone accepts that some people benefit let’s all work together, try and work out, which people benefit. Let’s work on case selection.
So we’ll put you on the spot then, when would you offer thrombolysis? Which patients would you offer it in and which circumstances would you also stent?
There’s no role for thrombolysis in anything other than the iliofemoral segment. So if it’s infrainguinal, proximal DVT, even if its severely symptomatic, the studies that actually you cause harm by attempting early thrombus removal. That’s the first important point.
Even if they have got severe symptoms, there’s always a role for initial conservative management, compression with elevation and a lot of these people have a dramatic improvement in their symptoms. If they don’t, and there’s an honest discussion, and the bleeding risk is low then potentially there is a role. But when there’s a treatment with a borderline benefit or the benefit is unclear, then I think what we’ve gotta do pick low risk patients, so low bleeding risk. We’ve got to choose teams and techniques with the highest risk of technical success. And we’ve got to pick people where we think the benefit is greatest, i.e. those that have the highest risk of PTS.
Whether or not you stent is very difficult. We had a case not so long ago where we had a very nice result from early thrombus removal, we stented, and the patients thrombosed again early and subsequently was identified to have triple positive antiphospholipid syndrome. Obviously there wasn’t the opportunity in the time to make that diagnosis prior to the decisions around the thrombus removal, so you end up stung and now this patient has a stent and can be very difficult to open up again. The advocates and the aggressive stenters would say, you can’t leave a significant stenosis after thrombus removal, otherwise they will rethrombose. Whereas others will say, if we go back to the early studies, like CaVent, very few, if any, people actually had stents, but actually their results were still reasonable.
I think once you get on the roller coaster of thrombus removal, it’s very difficult not to then proceed also to stenting, if you see a significant lesion, for example, at the May-Thurner point.(Wang et al. 2018; Meissner et al. 2012; Rollo et al. 2017) Final comment, I’ll make is that the use of recanalization and stenting for chronic PTS is a very effective technique. So another approach, if you’re not sure, is to manage them conservatively, but always have that up your sleeve, if they get significant PTS at six months, no earlier, then we could potentially consider recanalizing and stenting at that point.
Following thrombolysis, what duration of anticoagulation is required?
So the whole point of anticoagulation after DVT is to reduce the risk of propagation and pulmonary embolus, firstly, but also then to reduce the risk of recurrent VTE. The aims don’t really change if you thrombolyzed or if you put a stent in. Some people used to say, I put a stent in, we’ve treated the May-Thurner and that was the main cause of DVT, so we can stop the anticoagulation. That’s not the case. So it shouldn’t change and it shouldn’t be any shorter if you’ve thrombolize and put a stent in.
Now, whether it should be longer because you put a stent in that’s debatable. Some people have very aggressive anticoagulation protocols after stenting, but that’s to do with the stent rather than the DVT. So remember the aims, which are to reduce the risk of recurrent DVT and PE and to stop propagation of the current event.
18.3 Phlegmasia
Some patients may present with very profound, lower limb swelling. Pain and cyanosis with a threat to viability of the limb. Can you explain for us what phlegmasia is and an approach to treatment?
There’s two sorts phlegmasia that are described, but to be honest, I don’t think anybody has a detailed and robust understanding of what these actually mean. Phelgmasia alba dolens is the white leg, cerulea dolens is the blue leg and the severe, form a phlegmasia. Theoretically, cerulea dolens has a limb loss rate of 30-40%–severe limb threat, compartment syndrome, skin blistering, swelling, etc. The reality is that it’s often over-diagnosed, so you’ll see a lot of people saying I did venous thrombolysis for phlegmasia and it’s just a big swollen engorged leg.
The reason it happens is almost certainly a profound obstruction of venous outflow. So the venous blood in the leg cannot escape. You get this cycle of worsening pressure, leaking of fluid from the capillaries, increasing pressure on the soft tissues. Then that starts to threaten tissue perfusion and potentially if it’s bad enough this will threaten the actual arterial profusion of the leg as well. Presentation often includes iliofemoral DVT with non-palpable pulses and loss of sensation with out improvement on anticoagulation and elevation. Endovascular early thrombus removal is the first line with fasciotomies, with open thrombectomy as back up for salvage.(Erdoes et al. 2011; Thomas, Hollingsworth, and Mofidi 2019)
So that’s the sort of most severe and extreme form. I don’t think anybody has confidently linked the anatomical findings and features of a DVT to what the leg looks like. There was a patient I saw who literally had every deep vein acutely thrombosed from the IVC down to both lower legs and was almost asymptomatic. So we’ve got this very uncomfortable lack of understanding between the symptoms and the clinical and anatomical pattern of DVT.
18.4 Deep Venous Obstruction
18.4.1 Etiology
So finally, let’s move on to talk about the treatment of proximal deep venous insufficiency, both obstruction and incompetence. What are the common causes for deep venous obstruction? Thinking about post-thrombotic and non-thrombotic obstructions.
So again, the terminology is important. So it’s venous outflow obstruction. Obstruction implies that there’s a physiological issue causing the consequences. As opposed to occlusion, which is an anatomical term. So venous outflow obstruction, is essentially anything that reduces the ability of venous blood to escape the leg via deep venous channels will cause an obstruction.
And again, going back to a bit of physiology. Poiseuille’s Law talks about the flow rate being proportional to the fourth power of the radius. So it’s really interesting. A question to ask is that if you’ve got a two centimeter vein, how many, one centimeter veins would it take to carry the same potential flow as a single two centimeter vein?
The long story short is that it takes 16 one centimeter veins to carry the same amounts of potential flow as a single two centimeter vein. So it doesn’t take much of a narrowing to have a great potential impact on flow. Of course, most of the time, you don’t need that flow potential, it’s only an absolute extremes of circulatory stress that you’ll need that sort of potential, but it is interesting. And again, it also challenges when people say there’s great collaterals and that will be enough. Well unless they’re enormous, you need 16 of them to have the same potential blood carrying capacity.
So in terms of the causes, the most common by far is post-thrombotic disease. So when you’ve had a DVT, one of three things happens. If you’re lucky, the vein will recanalize completely. If you’re unlucky, it will obstruct completely. And if you’re somewhere in between, you’ll end up with partial stenosis and obstruction. What’s important is even if the vein is open, what you almost always lose in the post-thrombotic vein is venous compliance. It’s not the same compliant vein that can respond to demands and physiological need that you have, in a primary non-scarred vein.
Other potential causes are a non-thrombotic iliac vein lesion, or May-Thurner lesion. So the original paper, 1957, is very interesting reading.(May and Thurner 1957) There were a couple of Austrian pathologists who identified that a very high proportion of people, particularly those had left-sided DVT had, not only the overriding iliac artery causing compression, but they had a secondary tight fibrosis in the iliac vein.(Nazzal et al. 2015) So it’s not just the compression because any one of us in a certain position we’ll have a squashed vein. It’s the fact that there’s a secondary inflammatory fibrotic change, which is what’s causing the obstruction. So that’s a true May-Thurner or non-thrombotic lesion.(Liddell and Evans 2018; Rollo et al. 2017)
The other big group of patients of course, is malignant lymph node or retroperitoneal fibrosis related venous outflow obstruction. For example, a patient with a large retroperitoneal leiomyosarcoma may be involving the vena cava. In this case, these patients may require en bloc resection of the IVC and reconstruction with ringed PTFE, sized off the preoperative imaging.(Quinones-Baldrich et al. 2012; Fiore et al. 2012) But in the end, post-thrombotic by far was the most commonly diagnosed pathology.
18.4.2 Evaluation
We may see patients who come in with severe venous disease with skin changes, for example. When would you consider imaging the proximal deep veins in addition to infrainguinal superficial and deep veins of the leg and what are the best modalities to do this?
So we are really getting down to the importance of a detailed assessment of the entire superficial and deep venous system. Every patient with venous disease should have a whole leg infrainguinal duplex to start with—that’s deep and superficial veins. There’s no real role for just looking at superficial veins. So you need to understand the context. In terms of if their obstructed or if they’re refluxing. Again, remember that, reflux on a duplex, yes, all we see is arrows going in certain directions. But all reflux means is that after a calf augmentation maneuver, there is some retrograde flow—in a superficial vein, more than half a second and in a deep vein, more than one second. That’s all it means. So for example, you can have retrograde flow for 0.6 seconds in a saphenous vein, and that will be labeled as reflux for all the rest of the time that superficial vein is doing the right job, it’s returning the blood to the heart. So just be wary of interpreting what these arrows mean. For more, see Section 20.7.
In terms of how that affects your decision-making—one approach is to consider the overall burden of venous disease, such as those with venous hypertension. And what I try and do is draw a pie chart and say, you got venous hypertension, here are the different causes of your venous disease—that might include superficial reflux, deep venous reflux, deep venous obstruction, and other factors. You try and apply some clinical judgment as to what the different factors are.
Now, even if they’ve got significant, deep venous reflux and superficial venous reflux, there is still a role for treating superficial reflux in most of these cases. I still come across colleagues and other people who say, look, you shouldn’t treat the superficial veins if there’s deep reflux. But all the studies—EVRA, ESCHAR–have shown significant benefits, even if there’s deep flux.(Manjit S. Gohel et al. 2007; Manjit S. Gohel et al. 2018) So again, the key message is treat the superficial reflux if it’s there. However, if the patient has isolated deep reflux then management is limited to wound care and compression, often as high as 40-50mmHg. Some series have found that 70-80% will heal.(O’Donnell et al. 2014; Maleti and Perrin 2011)
Now, deep venous obstruction and looking for it is a different matter. There are again, lots of approaches, some people are very aggressive about evaluating the iliac veins—CTVs and IVUS on everybody. The problem is if you get super aggressive, then you start to over-diagnose and if you start to over-diagnose, you start to over treat and this all gets very messy.
I think the sort of people that have clear signs and symptoms of major venous outflow obstruction, particularly venous claudication, history of previous DVT, really disproportionate venous changes to the superficial and the infrainguinal imaging. Proximal obstruction can present with atypical proximal varicose veins in the mons pubis, perineum, buttock, high posterior/lateral thigh, abdominal wall. These findings are 93% predictive of deep venous obstruction proximal to the inguinal ligament.(Kurstjens et al. 2016) Those are the people that I would image.
And on the duplex imaging of the leg, if there are changes in the common femoral vein that make you think there is a proximal problem, particularly a loss of phasicity of flow then that’s pretty concerning for a significant venous outflow problem. In an unobstructed venous system, the common femoral vein should really reflect the right hearts, which has some phasicity. There should be transmission of that respiratory phasicity. So if that isn’t there, then you’re thinking, hang on, there’s something interrupting that transmission, which is almost always an obstruction somewhere. So those are the people I’d image, but I wouldn’t over image—because then you end up with a headache and a problem—Should I treat or should I not treat?
So you mentioned IVUS, what is intravascular ultrasound and what are the particular benefits of using this technique over venography alone?
IVUS is a 9F probe that is inserted into the vein and it gives you a 360 degree view in B-mode ultrasound—traditionally without color flow, just B mode—of the anatomical structures. What it’s very useful for is identifying venous anatomy, confluences, identifying the size of veins, so it allows you to plan sizes of stents. It really is an important adjunct to venography and other imaging modalities. We did our first 30 or so cases of deep venous stenting without IVUS and thought we were brilliant and IVUS was a waste of money. And then we started using IVUS and realized I can’t believe we were doing this without. Once you start using it, you suddenly realize that it’s a really useful adjunct. Recommended oversizing for vein stenting is 10-15% of largest diameter of adjacent vein.(Gloviczki et al. 2011; O’Donnell et al. 2014; Raju, Owen, and Neglen 2002; Raju, Darcey, and Neglén 2010)
In terms of when you use it, in some parts of the world it’s commonly used for diagnostic purposes, but beware of the risk of over-diagnosis. More commonly, almost routinely, IVUS is used for therapeutic, particularly when we’re stenting deep veins to plan our landing zones. When CTA/MRA shows compression, it must be confirmed with IVUS prior to treatment. IVUS has far greater sensitivity and specificity and must show a cross-sectional surface area reduction of greater than 50%.(Gagne et al. 2018; Forauer et al. 2002)
You talked about over-diagnosis. Can you talk us through some of the decision-making processes that you go through when you’re assessing a patient who has a deep venous obstruction?
There are lots of patients that have this anatomical change, the number of referrals I get from people who have done a CT and they’ve picked up a problem. The most important thing is the clinical status and the clinical picture. So have they got symptoms—go about right at the beginning of the podcast—have they got symptoms? Have they got complications? If they haven’t got significant symptoms and they haven’t got significant complications then there’s not really an indication for treatments.
So leg swelling was initially, frequently pushed as, oh you’re swelling will get better, if we get rid of your obstruction. That’s only the case in probably less than 50% of patients. The reason for that is that, yes the original etiology for the swelling may well have been venous, but you almost always get a secondary lymphatic dysfunction when you’ve had swelling, for whatever reason—whether it’s heart failure, whether it’s venous, the lymphatic system gets damaged. And so even if you get rid of the original cause, the lymphatic damage persists, of course, and the swelling persists.
The symptoms are very important and in terms of complications, if somebody has intractable ulceration, et cetera, these are all important indications. But a bit of skin change, a bit of mild swelling, careful case selection is very important for these procedures.
18.4.3 Management
18.4.3.1 Endovascular
There is variability in the availability of stents for venous obstruction. However, closed cell braided stents (i.e. the Wallstent) have been around for many years and has the most data related to long term durability.(Gagne et al. 2019) These stents have the least radial force at the ends, so it is recommended to extent 1-2cm beyond the venous obstruction. In cases of proximal iliac vein obstruction, this may require extending into the IVC 1-2cm which may cross, or “jail” the contralateral iliac vein. When jailed, the rate of DVT on that side has been reported as high as 10%.(Murphy et al. 2017; Le et al. 2018)
So following a deep venous recanalization and stenting, what surveillance do you offer for these patients?
Surveillance has been evolving. The first availability CE (UK version of FDA) marked deep venous stents in the UK was around 2012. A few services across the country really got started at a few centers in 2012, 2013. Initially there was an early scan and then a scan maybe at six weeks and three or six months down the line.
I think we realized that in general, the people that developed problems, often develop them very early. So we are scanning these people the day after the intervention—obviously there’s intraoperative quality control and venograms and scanning—but the day after the intervention to ensure that there’s no early thrombus problems. Then we scan a couple of weeks after to make sure that there’s nothing that’s happened early, because there’s an opportunity to re-intervene, to balloon, to correct any technical issues, at that point. After that point, it’s usually six weeks, three months, six months, and then annually thereafter.
So that’s a sort of protocol that we have and in general, what we’ve seen is that people that develop problems tend to develop them relatively early. So once you get to a year, then in general, the patency rates are very good. In our center, the the chronic PTS stenting primary patency rates at around three years are over 80%-85%. Of course, there are some that have problems, but it’s important to remember that, even those that have thrombosed, they generally go back to the level of symptoms they have prior to intervention. Which is very reassuring. The last thing you want to do is to make people worse with a novel intervention.
And so what about your anticoagulation and antiplatelet regime for these patients?
There was a systematic review done a few years ago where all of the published literature for deep venous stenting was reviewed and I think the authors identified 28 different regimens for anticoagulation of the stenting.(Notten, Ten Cate, and Ten Cate-Hoek 2021) The honest answer is nobody knows, our approach is to have low molecular weight heparin as the primary anticoagulant for the initial two week period. And then at the two week point, they undergo a stent. If there’s no issues, they get transitioned to a DOAC.
In addition, the patients get six weeks of clopidogrel as an anti-platelet. And again, the reason for that is that it’s a foreign material into the vein. Yes, the role of anti-platelets in preventing venous thrombosis is very limited but there has to be some platelet related activity and platelet activation involved there. So it makes logical sense to have some anti-platelet activity. Of course the downside is that there’s an increasing bleeding risk. These are the constant tightropes that you’re walking with these patients.
Take a Listen
Check out our episode with Drs. David Gordon and David Williams on a recent publication looking at the evolution of in stent restenosis and the classification of thrombus forming in venous stents.
18.4.3.2 Surgery
We’ve talked about endovascular and endovenous treatments, but is there a role for open surgery in these patients?
So in the iliac segment, very rarely. In some patients, you can do PTFE reconstructions and bypasses. And of course the traditional operations of Palma-Dale(Palma and Esperon 1960) bypass and May-Husni(Shaydakov, Porembskaya, and Geroulakos 2015) type procedures. They all sounded very elegant in the books, but the reality is a great saphenous vein going across the lower abdomen to the other side is not really going to sort the problem out in a durable way for all sorts of obvious reasons—the size of the vein, the pressure and all that sort of stuff. So there’s really very limited role for those sorts of procedures.
Now, the one area where there may be a role for open reconstruction is in the common femoral vein. The consistent observation is that good inflow is absolutely imperative to get good outcomes in these patients. And sometimes if the common femoral vein has got a lot of scarring, then it’s very difficult to reconstruct that inflow endovascularly. So a number of authors have advocated the use of endophlebectomy, opening up the common femoral vein, and cutting out the scarring and the tribulations, putting a patch on it. Sometimes even putting an AV fistula—a little six millimeter graph from the common femoral artery onto the vein to really drive the flow through the stent. It’s a pretty complicated operation and you can imagine you’re dissecting down and there’s lots of little veins everywhere and lots of lymphatics. The wound complication rate is very high.
So really very limited role only—the endovascular approach is really the way forward for these patients.
18.5 Pelvic Congestive Syndrome
18.5.1 Presentation
So finally, let’s talk about pelvic congestion syndrome. What is pelvic congestion syndrome and how does it present?
So it often doesn’t present anywhere near a vascular surgeon. There are a number of women who present with these chronic heaviness and dragging symptoms in the lower abdomen. There may be some association with menses, there’s often dyspareunia and a whole variety of other symptoms.
There may be associated vulvar varices or posterior buttock and thigh varices all as a result of pelvic venous incompetence. Knowing the proximal anatomy of the saphenous vein tributaries is important, as the pudendal vein tributary connects vulvar veins and inferior gluteal vein connects to the posterior buttock.(Iafrati and Donnell 2019) But it’s a complicated field—there are some people that have pelvic symptoms, there are some people that have the varicose veins or some will have a combination of the two. Almost always they will be seen and initially assessed by the gynecology teams rather than coming to the vascular surgeons.
18.5.2 Evaluation and Management
When we do see these patients, are there any treatment options available for them? And when would you consider treating?
In a highly selective way—this is venous disease in a nutshell—the association between anatomical changes and clinical symptoms is ropey at best. In terms of postpartum women, an enormous proportion of these women have got venous reflux in the pelvis—if you look hard enough. so the problem is similar to that of May-Thurner syndrome, if you start looking hard enough, you start identifying these symptoms and then you lose the ability to really discern who’s going to benefit most.
So again, I would go back to clinical symptoms as the single most important thing. If they’ve got severe clinical symptoms majorly affecting their quality of life and associated significant venous changes, then those people to try to intervene on. It’s not necessarily a benign procedure. Pelvic vein embolization involves implantation of coils. There’s concerns about non-targeted embolization as coils have ended up in lungs. There are a number of people with unknown nickel allergies that have problems with these coils. So again, it’s not an area to be over aggressive. So careful case selection is important. So again, a quick plug for the ESVS guidelines. There is a very good section on pelvic venous disease assessment.(De Maeseneer et al. 2022)
What’s very important is again, to differentiate between pelvic congestion syndrome and pelvic origin varicosities. One thing that is certainly being advocated is that if the varicose veins are coming from the pelvis, but there’s no pelvic congestion syndrome, it’s perfectly reasonable just to deal with the visible varicosities from below—with some foam sclerotherapy or other treatment from below, rather than being super aggressive embolizing from above. But I think anybody who’s involved in managing this really needs to work closely with the gynecologists. There are gynecological diagnoses that need excluding before we start to address the venous disease. And there are a number of validated questionnaires and other assessment tools that are probably quite important. So not for the faint-hearted.
18.6 Superior Vena Cava (SVC) Syndrome
SVC syndrome is an acute presentation of head and neck venous congestion often due to SVC obstruction. This can be intrinsic due to indwelling devices or extrinsic due to malignancy or mediastinal fibrosis (half of benign cases).(Kalra, Bjarnason, and Gloviczki 2019; Rice, Rodriguez, and Light 2006; Parish et al. 1981)
18.6.1 Management
Angioplasty and stenting are first line treatment for benign etiology.(Rizvi et al. 2008; Sheikh et al. 2005) Angioplasty alone may be sufficient, but stenosis refractory to angioplasty may require stenting. SVC syndrome with failed endovascular management in reasonable operative candidates can undergo open reconstruction with large diameter prosthetic graft or spiral vein graft.(Doty, Flores, and Doty 1999) However, restenosis in open repair can be as high as 15%.(Kalra, Sen, and Gloviczki 2018; Sfyroeras et al. 2017)
SVC syndrome secondary to malignancy, bronchogenic or lymphoma, is often most effectively treated with palliative radiotherapy with good response.(Talapatra et al. 2016) Endovascular or open recannalization is often reserved only for those with severe symptoms refractory to radiation or chemotherapy.(Higdon and Higdon 2006) Lymphedema pumps can help with symptom management as well.
18.7 Lymphedema
Here we will discuss lymphedema of the lower extremity. This is a broad topic, but the management decisions are relatively straightforward and knowledge is required for examinations. For upper extremity lymphedema, see Section 3.8
18.7.1 Demographics
18.7.1.1 Etiology
Lymphedema can be thought of as a primary dysfunction of the lymphatic channels or the secondary result of a disease that results in the destruction of lymphatic flow. Causes of secondary lymphedema include filariasis, which is endemic to parts of South America.(Pfarr et al. 2009; Shenoy 2008)
18.7.1.2 Presentation
The management of lymphedema is determined primarily on its clinical stage at presentation.(Grada and Phillips 2017) The staging for lymphedema is as follows:
| Lymphedema Stage | Description | Symptoms |
|---|---|---|
| 0 | Sub-clinical | No swelling, heaviness or discomfort |
| 1 | Spontaneous Reversible | Swelling improved with limb elevation |
| 2 | Spontaneous Irreversible | Pitting and swelling, not improved with elevation |
| 3 | Lymphostatic elephantiasis | Skin hardening, non-pitting edema, verrucas changes, recurrent infection |
18.7.2 Evaluation
On physical exam, a classic finding is Stemmer’s sign, which is a thickened skin fold at the based of the second toe/finger. The sign is positive when the tissue is hardened and cannot be lifted.(S. G. Rockson et al. 1998; Stanley G. Rockson 2019)
Lymphedema is most often diagnosed based on clinical presentation and physical exam. Lymphoscintography can be used to confirm the diagnosis in complex presentations and would demonstrate dermal back flow, absent or delayed transport, crossover filling, absent or delayed visualization of lymph beds.(Stanley G. Rockson 2019; O’Donnell, Rasmussen, and Sevick-Muraca 2017)
18.7.3 Management
Treatment is best initially managed with combined decongestive therapy (CDT) which includes an intensive reductive phase (4-8wks), followed by life long maintenance, often with specific compression garments.(Grada and Phillips 2017) CDT in the setting of heart failure has been reported to lead to volume overload.(Lawenda, Mondry, and Johnstone 2009)
In extreme cases, after CDT therapy has been instituted for at least 6 months and the patient has persistent refractory symptoms, surgery may be used for reconstruction or debulking.(Grada and Phillips 2017; Baumeister et al. 2016)